Introduction
The US Department of Defense (DoD) and other government agencies are investing in wearable sensors for monitoring the health and readiness of service members (SMs) and first responders. Wearable sensors (“wearables”) are broadly defined as self-contained devices that combine typical characteristics of point-of-care systems with onboard analytics and wireless connectivity (Ates et al., 2022). These devices measure several physiological signals, from physical activity to heart rate (HR) and peripheral oxygen saturation (SpO2). Wearables are available in a variety of configurations, such as watches and fitness bands, chest straps, rings, and even earbuds or eyeglasses (Ates et al., 2022). Flexible sensing technology in the form of textiles, bandages, or patches is also being applied to monitor biofluids and certain biosignals, such as the electrocardiogram (ECG) (Ates et al., 2022).
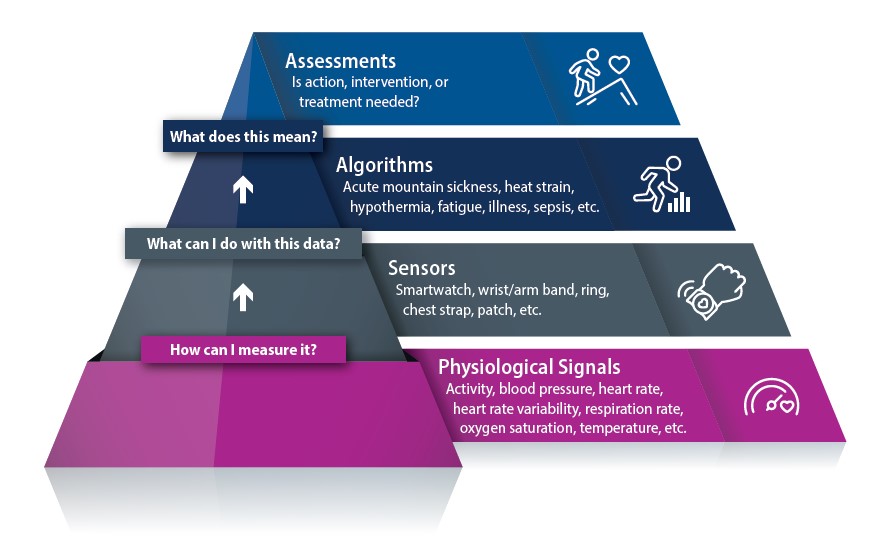
Wearables can continuously monitor individuals during training and deployment. This monitoring takes several forms, including (1) evaluating immediate health status (e.g., heat strain, hypothermia, altitude sickness, chemical or biological exposures), (2) assessing longer-term health indicators (e.g., performance optimization, fatigue/stress/recovery, and illness detection), and (3) triage and remote symptom observation (e.g., major trauma and sepsis) (Friedl, 2018). Although researchers and medical personnel may want access to high-resolution data over weeks to provide a comprehensive assessment of health, care for SMs and first responders requires that the rich information from wearables be distilled into binary alerts (Figure 1). This distillation necessitates that the raw physiological data move quickly and securely from skin to data processing and display in non-ideal situations (e.g., during high levels of physical activity or in resource-constrained environments). Algorithms clean and combine information from several physiological signals to indicate risk level, and the results of individual algorithms can aggregate into actionable information to determine whether someone is fit for duty or can continue to perform a given task (Friedl, 2018).

To meet the needs of SMs and first responders, wearables must be robust (water resistant, able to withstand crushing forces, etc.); have an extended battery life and easy charging solution (especially for deployed scenarios); be able to communicate over military networks; and be small, lightweight, and comfortable while not interfering with job duties or any equipment being worn (Buller et al., 2021; Friedl, 2018). Unfortunately, there are no DoD-wide or common first responder requirements definitions for wearable sensors and monitoring platforms. This leaves the burden of selecting wearables on researchers, vendors, and leaders within the military and first responder communities and has resulted in a collection of disparate systems that are either used within a specific population or fulfill the needs of niche application. Optimizing wearables’ usefulness for monitoring the health and safety of SMs and first responders will require definition of common data elements and system attributes.
Literature Review—Concepts of Operation
To frame requirements for wearable sensors and platforms for the SM and first responder communities, we highlight recent examples below of how wearables are currently being leveraged. We review requirements for six different concepts of operation (CONOPS), including immediate (e.g., heat strain and hypothermia and acute mountain sickness) and longer-term (e.g., fatigue and recovery and illness detection) health status, triage, and remote symptom observation (e.g., major trauma and sepsis). Although we focus on CONOPS for SMs and first responders, several of these examples relate to the general public as well. This literature review is not meant to be all-encompassing, and we did not establish a formal review protocol. We focused on recent publications and articles (2019 to date) that were specific to the military or first responder populations and on wearable sensors that were commercially available and could be fielded.
Immediate Health Status—Heat Strain and Hypothermia
Exposure to extreme environmental conditions can affect the body’s ability to maintain homeostatic conditions (i.e., core temperatures between 36 and 38°C). Conducting physical activity in hot or humid environments, or when wearing personal protective equipment (PPE), can interfere with the body’s ability to dissipate heat. Water loss, HR, and core body temperature (Tc) climb, which can result in heat-related illness (HRI). In the case of hypothermia, the body attempts to generate heat through a shiver mechanism. Blood flow to the skin is decreased, and HR and respiration rate (RR) initially increase. If exposure to cold temperatures continues and the body cannot counteract heat loss, muscle temperature drops, activity level (including shivering) drops, and Tc falls. Models can accurately predict Tc if activity level, environmental conditions, and material properties of the clothing are well characterized (Buller et al., 2021; Dolson et al., 2022; Friedl, 2018; Shakerian et al., 2021). However, using population-level physiological information can render these models inaccurate on an individual level (Dolson et al., 2022; Friedl, 2018; Runkle et al., 2019; Shakerian et al., 2021).
Accurate measurements of Tc are the most straightforward way to assess HRIs or hypothermia. Invasive measurements (i.e., esophageal, rectal, gastrointestinal) are the most accurate, but are impractical for continuous measurements outside of the clinic (Dolson et al., 2022; Roossien et al., 2021). Of noninvasive techniques, tympanic (i.e., ear) measurements most closely reflect Tc because the hypothalamus is responsible for maintaining Tc (Roossien et al., 2021; Shakeel et al., 2022). Tympanic measurements are typically taken with infrared (IR) sensors, which can be incorporated into earpieces (e.g., Cosinusso oTemp) for continuous measurement that does not interfere with helmets or other PPE (Roossien et al., 2021; Shakeel et al., 2022). The probes must be properly shielded from the environment to be accurate, and individual correction factors may be needed if the individual uses an off-the-shelf device or wears PPE (PPE can result in local warming around the ear) (Roossien et al., 2021). Measuring skin temperature (Tskin) is another non-invasive option, although Tskin typically reflects local environmental conditions. If measured under a garment in regulated conditions (e.g., a space suit), assessing Tskin at multiple points on the body can be effective (Palacios et al., 2020). Additionally, when combined with HR, Tskin can be used to estimate rectal temperature (Shakerian et al., 2021). Dolson et al. recently reviewed technologies and methods for measuring Tc and predicting heat strain (Dolson et al., 2022).
HR, RR, electrodermal activity (EDA), accelerometry, and Tskin may also be used alone or in combination to assess risk for HRI (Buller et al., 2021; Friedl, 2018; Runkle et al., 2019; Saidi & Gauvin, 2023; Shakerian et al., 2021). Multimodal algorithms can achieve high accuracy (Buller et al., 2021; Friedl, 2018; Saidi & Gauvin, 2023; Shakerian et al., 2021), and several prototype garments for specific populations of workers that incorporate some or all of these types of sensors have been proposed; see Saidi and Gauvin (2023) for a comprehensive listing. However, sustained high HR alone measured using smartwatches (Runkle et al., 2019), armbands (Buller et al., 2021), or chest straps (Buller et al., 2021; Friedl, 2018; Saidi & Gauvin, 2023) can also be used to indicate heat strain. For example, the ECTemp™ algorithm uses HR to accurately predict Tc under a variety of conditions experienced by active-duty SMs (Buller et al., 2021; Friedl, 2018). Several monitoring systems for military personnel have incorporated this algorithm (e.g., the ARMOR Heat Monitor developed by the Netherlands Armed Forces) (Buller et al., 2021). Although Tc or HR alone can be used to indicate risk for HRI, this is insufficient for detecting hypothermia because large drops in Tc have been observed without consequence and HR is within physiologically normal ranges (Friedl, 2018).
Immediate Health Status—Acute Mountain Sickness
It is critical to monitor the health of individuals operating in high-altitude environments because the onset of acute mountain sickness (AMS) can happen quickly and be life-threatening without treatment (e.g., stopping ascent or administering medications or oxygen). AMS is difficult to diagnose because the symptoms are nonspecific (headache, vomiting, fatigue/weakness, etc.) and the pathophysiology is poorly understood (Muza, 2018). Although models have been developed to assess risk for developing AMS (Muza, 2018), these population-based models are insufficient for knowing whether an individual will develop symptoms. Activity intensity, acclimatization, and other physiological factors, such as age and respiratory illness, can affect risk (Muza, 2018; Tang et al., 2022).
Artificial intelligence and machine learning (AI/ML) modeling techniques can combine periodic vital sign measurements with demographic information and altitude level to evaluate an individual’s risk of developing AMS (Tang et al., 2022). Although lower SpO2 is predictive of AMS, findings related to the relationship between blood pressure (BP), HR, and heart rate variability (HRV) and AMS are mixed (Muza, 2018). However, the consensus is that continuous measurements are better at distinguishing risk than spot checks of vital signs (Muza, 2018).
Although wearables can continuously measure vital signs, SpO2 in particular may be difficult to obtain using commercially available sensors. SpO2 is traditionally measured when an individual is at rest using a finger-worn sensor or ear clip that operates in transmissive mode, but this is impractical for continuous wear (Telfer et al., 2017). Wearables using reflectance-based optical sensors may not have the needed accuracy to measure the physiological changes associated with AMS. Motion artifact at the wrist leads to high inaccuracy in the SpO2 measurements obtained using smartwatches (Schiefer et al., 2021; Telfer et al., 2017). For example, the Garmin Fenix 5X Plus (Garmin Ltd., Switzerland) smartwatch measured higher SpO2 values than tools using arterial blood gas analysis, leading to an underreporting of hypoxia (Schiefer et al., 2021). Monitoring cerebral blood flow is of interest because headache is a classic symptom of AMS (Muza, 2018). Sensors worn in other locations (e.g., forehead) may also have better signal quality, but packaging and powering these devices for wear in harsh environmental conditions remain a challenge (Telfer et al., 2017). Optical sensors can accurately monitor other health status information, such as HR and HRV during sleep (Castiglioni et al., 2022).
Longer-Term Health Status—Fatigue and Recovery
Fatigue management for SMs received prominent attention after fatigue was the root cause of the deaths of 17 sailors and damage to two warships in 2017 (Brager et al., 2022). Fatigue can result from a variety of sources, from disrupted sleep to high levels of physical exertion, cognitive overload, and so on. These circumstances are unavoidable in current military contexts (Brager et al., 2022). Assessment strategies for fatigue rely on questionnaires or surveys, performance-related metrics (e.g., motor performance on specific tasks), models of the circadian cycle, or behavioral indicators (e.g., yawning, blinking, and head nodding) (Adão Martins et al., 2021; Brager et al., 2022; Friedl, 2018; Kniffin et al., 2021; Kodithuwakku Arachchige et al., 2022). These strategies lack specificity, especially for early detection of fatigue at the individual level (Adão Martins et al., 2021; Kniffin et al., 2021). Changes in physiological signals can indicate fatigue, and supervised AI/ML models that combine data from several sensors can achieve high accuracy. Fatigue is multifaceted, and there is consensus that longer-term studies conducted outside of a laboratory environment are needed and that greater standardization is required when designing approaches to assess fatigue (Adão Martins et al., 2021).
Electroencephalogram (EEG) measurements are considered the gold standard for assessing and diagnosing vigilance and drowsiness (Adão Martins et al., 2021; Friedl, 2018; Kniffin et al., 2021). Wearable headband or cap-based EEG systems can measure changes in spectral power bands and event-related potentials (Adão Martins et al., 2021; Kodithuwakku Arachchige et al., 2022). Inertial measurement units or near-infrared spectroscopy sensors can be used with EEG sensors to monitor head movement and cerebral blood flow, respectively, to increase detection accuracy (Adão Martins et al., 2021). Optical eye-tracking and electrooculogram systems have been used to unobtrusively monitor fatigue and provide information about cognitive state (Friedl, 2018; Kodithuwakku Arachchige et al., 2022), but commercially available systems are not accurate enough for use with SMs operating in the field (Schweizer et al., 2022).
Other groups have used HR, HRV, RR, EDA, Tskin, and electromyogram signals either singularly or in combination to predict physical/mental fatigue or drowsiness (see Adão Martins et al., 2021, for a comprehensive review). HR and RR increase with workload, and HRV also increases greatly because of heightened parasympathetic activity (Kniffin et al., 2021; Kodithuwakku Arachchige et al., 2022). Several of these cardiorespiratory biomarkers also can be used to assess circadian misalignment (Brager et al., 2022; Friedl, 2018). Highlighting studies that were conducted with military personnel, Markwald et al. found that both the Oura ring (Oura Health Ltd., Finland) and the ReadiBand wrist-worn device (Fatigue Science, Canada) can accurately measure total sleep time, sleep efficiency, and daily activity (Brager et al., 2022; Markwald et al., 2022). Total sleep time is correlated with self-reported measures of fatigue and exhaustion (Markwald et al., 2022).
Longer-Term Health Status—Illness Detection
The COVID-19 pandemic sparked interest in remote symptoms monitoring and detecting illness before symptom onset. Several recent studies and review articles have focused on using wearables to detect influenza (Radin et al., 2020) and influenza-like illnesses, including COVID-19 (Cheong et al., 2022; Mitratza et al., 2022; Nestor et al., 2021). Most of these analyses have been done retrospectively using data from wrist-worn wearables (Fitbit devices and the Apple watch are most frequently used) (Cheong et al., 2022). AI/ML models have been applied to the data using participant-reported symptoms and diagnostic data for labeling (Mitratza et al., 2022). Most models included some measure of changes in resting HR (Cheong et al., 2022; Mitratza et al., 2022). Other metrics that showed good discrimination for detecting influenza-like illnesses in some studies were changes in HRV, RR, SpO2, Tskin, and activity level (Cheong et al., 2022). Generally, including more metrics improved the detection accuracy; however, these models do not achieve high sensitivity for detecting a specific respiratory virus or influenza-like illness (i.e., influenza versus COVID-19) using wearables data only, especially in the presymptomatic phase (Mitratza et al., 2022; Nestor et al., 2021). The models are likely detecting physiological changes that are indicative of an immune response and track with symptom severity.
Focusing on a few unique studies, Natarajan et al. were among the first to show that resting RR, HR, and HRV measured with smartwatches (i.e., Fitbit devices) could be used for the early detection of COVID-19 (Natarajan et al., 2020). Temple et al. also found that HR and HRV could be used to detect influenza before symptom onset, and that continuous assessment could be achieved by standardizing these metrics for the known influences of physical activity (Temple et al., 2022). The TemPredict study focused on the addition of temperature and used data from the Oura ring to accurately identify (82 percent sensitivity) COVID-19 onset (Mason et al., 2022). Performance was best when all data streams (HR, HRV, RR, metabolic equivalent of task, and dermal temperature) were included, and the addition of dermal temperature (especially during sleep) improved performance by nearly 5 percent. The Rapid Analysis of Threat Exposure study combined data from Garmin smartwatches and Oura rings to predict COVID-19 in SMs an average of 2.3 days before diagnostic testing (Conroy et al., 2022). This study highlighted the differences between hospital-grade measurements of SpO2 and temperature and those measured from a wearable, finding that the features could not simply be substituted in models developed from clinical data. Pivoting from HR and temperature, Miller et al. specifically focused on RR (measured using the WHOOP strap) and derived several measures to capture nighttime RR changes over different time scales, achieving a classification accuracy of 80 percent by the third day of symptoms (Miller et al., 2020).
Triage and Remote Symptom Observation—Major Trauma
Patient triage is critical for providing timely life-saving emergency care, especially in mass casualty scenarios where first responders need to manage large numbers of people with little time for preparation. Trauma patients are typically evaluated using vital sign measurements, and several existing tiered scales can be used to prioritize care (Nino et al., 2020). This method of triaging has several problems that wearables can address, including (1) monitoring vital signs continuously and quantitatively after initial admission to detect changes in health status and (2) supplying additional information or higher precision measurements.
Once an individual is assessed and assigned to a priority group, vital signs are not currently routinely checked to determine whether their health status changes while they are waiting for care (Nino et al., 2020). Additionally, priority group assignments are not evenly distributed over the triage scales used, so it is difficult for medical personnel to accurately determine who is in greatest need of care at that moment (Nino et al., 2020). A survey of first responders indicated that pulse (highest priority), BP, temperature, RR, SpO2, peripheral vascular perfusion, metal state, and ECG waveform characteristics were important measurements to obtain (Nino et al., 2020). Battlefield medics prioritized BP, HR, and SpO2 measurements for triage (Carius et al., 2022). Several research and commercially available systems have been proposed for triage applications (Ng & Bennett, 2022; Nino et al., 2020), but most of these are focused on HR, RR, and temperature and omit BP. Hemorrhage is the most common cause of death following major trauma and is mainly assessed through BP and HR measurements (Convertino et al., 2020; Zia et al., 2020). BP is difficult to measure under battlefield conditions because of the noisy and chaotic environment and lack of access to equipment (Carius et al., 2022). Medics often rely on arterial palpitation, which is not an accurate estimator of hypotension and overestimates BP in patients with the lowest actual pressures (Carius et al., 2022). There is a need for comprehensive sensing platforms that are accurate, robust, and easy to apply when patients are being evaluated and moved.
Simply tracking vital signs measurements, even continuously, is inadequate for improving current methods of triage. Medics need algorithms to synthesize the vital signs information into a triage score so they can properly prioritize patients. Additionally, medical personnel need alerts when an individual’s status has changed. A few algorithms have been proposed for objectively assigning and dynamically shifting individuals waiting to receive care, including the Dynamic Grouping and Prioritization Triage Algorithm, eTriage, Electronic Triage System, and the Soterion Rapid Triage System care (Nino et al., 2020). The algorithms use vital signs measurements, demographic information, pain level, and primary injury or compliant care (Nino et al., 2020). Convertino et al. suggested an improved method of triaging and tracking trauma patients over time using compensatory reserve measurement (CRM) (Carius et al., 2022; Convertino et al., 2020; Zia et al., 2020). This method focuses on hemorrhage; vital sign changes are a lagging indicator of hemorrhage. CRM is assessed using continuous measures of change in the arterial pressure waveform morphology, which can be measured outside of clinical environments using optical sensors (Convertino et al., 2020). Zia et al. demonstrated a wearable sensing system for assessing CRM that achieved similar results to gold-standard monitoring tools for assessing hemorrhage (Zia et al., 2020). They also found that time-domain HRV measures were sensitive indicators of hemorrhage (Zia et al., 2020).
Triage and Remote Symptom Observation—Sepsis
Sepsis is a life-threatening condition resulting from an acute infection. Studies related to using wearables for sepsis monitoring mainly focused on remotely acquiring vital signs data within a clinical environment (Ghazali et al., 2022; Joshi et al., 2022) and using this data with AI/ML models to predict sepsis (Choi et al., 2022; Sadasivuni et al., 2022). Remote monitoring and prediction using wearables are especially important in low- and middle-income countries (LMICs) where access to clinical equipment and trained medical staff is limited (Garbern et al., 2019; Ghiasi et al., 2022). One prospective study used a wearable patch sensor (Sensium, The Surgical Company, United Kingdom) that measured HR (from ECG), RR (from impedance techniques), and temperature (from a probe placed under the armpit). The sensor issued alerts if one or more of these vital signs was outside of the expected range. Of the 50 patients monitored, 18 patients had alerts, and 2 of the patients went on to develop sepsis (Joshi et al., 2022). This same sensor warned hospital staff of a patient’s deteriorating condition that resulted in sepsis (Ghazali et al., 2022). Garbern et al. also used a patch sensor (VitalPatch, Vital Connect, United States) that measured HR (from ECG), RR, and Tskin in combination with a mobile app (physIQ, Inc., United States) to monitor patients with suspected sepsis who were admitted to a representative LMIC emergency department (Garbern et al., 2019). They found that clinically significant vital sign changes could be detected hours before they were entered into the patient’s record. Timely treatment is critical for preventing septic shock and further deteriorations in health. The HR and RR measurements from the wearable also agreed with the nurses’ manual management, and data could be transmitted 97 percent of the time.
In terms of sepsis prediction, Choi et al. explored using the HiCardi (Mezoo Co, Ltd., Wonju-si, Gangwon-do, Korea), which is a wearable patch sensor that measures HR (from ECG), RR, and temperature in combination with vital signs measurements taken hourly to predict sepsis (Choi et al., 2022). This strategy effectively predicted sepsis up to 9 hours before onset. Ghiasi et al. used HR and HRV metrics extracted from a single-lead wearable ECG sensor (ePatch®, Delta Electronics, Denmark) in a ML model and were able to accurately predict mortality from sepsis (Ghiasi et al., 2022). They found average HR and nonlinear measures of HRV to be most predictive. Sadasivuni et al. also explored an ECG-only solution and achieved 95 percent accuracy in terms of sepsis prediction within 1 hour of onset (Sadasivuni et al., 2022). When combined with basic demographic and comorbidity information from electronic medical records, sepsis could be predicted up to 6 hours before onset.
Results
For the CONOPS described, we summarized the spectrum of physiological signals that were measured and the sensors used to make these measurements (Table 1).
We then inventoried the sensors from the referenced studies. We summarize the defining characteristics for each of these sensors in Table 2 (note: we used the specifications for most-recent device model). We also included popular wearables used by consumers and researchers (if specific models were not provided) and completed the same inventory. We included 18 sensors: 10 smartwatches/wristbands, 1 armband, 1 ring, 1 chest strap, and 5 patch sensors.
Discussion
When carefully selected, wearables can provide valuable insights into the immediate and long-term health status of SMs and first responders. The wearables wirelessly transmit signals to a hub, which often forwards the signals to a cloud-based endpoint for further processing and storage. If the hub has display capabilities (i.e., mobile phone, tablet, or desktop computer), it can display signals from the wearable. In this way, wearables can create a historic record of an individual’s health and actionable information based on immediate health threats.
Across several of the CONOPS explored, researchers acquired physical activity (or gait or posture), HR, HRV, and temperature (core or skin) from wearables and used these as inputs to predictive models. However, domain-specific needs drove the selection of wearables. When immediate feedback to an individual or leadership was required (HRI, hypothermia, AMS, etc.), the “health signal” (HR, temperature, etc.) needed to be acquired, processed, and transmitted in near real-time so that an intervention could be administered quickly. These CONOPS prioritized communication and the display of actionable information. These CONOPS also needed greater accuracy in event classification so symptoms did not progress to an acute state and to avoid unnecessary interventions. Many of the sensors and systems explored for these CONOPS were still in the prototype phase because commercially available systems did not provide the needed accuracy or on-board (versus cloud-based) algorithms for the specific use case.
Triage and remote symptom monitoring applications also prioritized accuracy and data availability. Although monitoring time is more extensive than short-term health status applications, individuals are not active. All of the reviewed sepsis studies used commercially available patch sensors that combined several vital sign measurements including temperature either via skin or axillary probes for fever monitoring and ECG for monitoring HR, HRV, and arrythmias; ECG (versus optical techniques) is considered the gold-standard measurement.
For longer-term indicators of readiness (fatigue/recovery, illness detection, etc.), some of the same health signals were acquired, but the data did not need to be immediately available. Instead, requirements focused more on data quality and integrity for long wear periods, and the form factor of the device, battery life, and ease of use were prioritized. Even though wearables-based databases are extensive, many of the datasets have large gaps in data and must be discarded when developing models. To establish good baseline data and relevant predictions of health risks, it is critical to minimize potential for data loss by ensuring that the device is comfortable, keeps the user engaged, and does not need to be frequently recharged (i.e., devices are often forgotten on chargers).
The wearable device market continues to grow rapidly. The data from wearables need to be benchmarked against gold-standard measurements to assess the inaccuracies incurred by moving away from clinical-grade equipment (Friedl, 2018). Identifying the causes of poor data quality and quantifying the noise floor of these sensors is important when developing algorithms and models that use the wearables to make health predictions (Zia et al., 2020). Although not listed explicitly in the CONOPS described, access to less-processed or higher-resolution data can help researchers develop a more robust feature set that is independent of the device used for acquisition (e.g., Garmin versus Fitbit smartwatch) and accounts for noise sources (e.g., wearables versus clinical-grade equipment). Additionally, researchers can tailor features to the population being monitored (e.g., injured older adults versus elite athletes) to describe their health status more accurately. Although wearables are a powerful tool, before using them to make health assessments, researchers should carefully think through data requirements and management plans.
This literature review identified several common data elements (e.g., physical activity, body position, HR, HRV, and temperature) used across several CONOPS. Additionally, this literature review identified sensor features that should be considered when selecting devices for these populations (e.g., accuracy, comfort, battery life, and timely feedback). Together with security considerations, these findings can shape DoD and first responder requirements for wearable sensor platforms. We recommend defining separate requirements for platforms that are predominantly used in resource-rich (e.g., garrison setting or civilian use cases) versus resource-constrained (e.g., in the field) settings as well as those used predominantly for short (e.g., training in a hot/humid environment) versus longer-term (e.g., general health) monitoring. Taking this approach ideally builds a flexible wearables toolbox that can be scaled and drawn on to satisfy the requirements of several CONOPS.
Acknowledgments
The Defense Advanced Research Projects Agency sponsored and contributed to RTI International’s recent research using wearables to detect viral illness before symptom onset under the SIGMA+ program. The Joint Program Executive Office for Chemical, Biological, Nuclear, and Radiological Defense has sponsored RTI’s wearables testing with end users. The views, opinions, and findings expressed are those of the author and should not be interpreted as representing the official views or policies of the Department of Defense or the US Government.
RTI Press Associate Editor: Jules Payne