Introduction
Stress is consistently associated with a myriad of physical and mental morbidities, as well as mortality (Russ et al., 2012). Additionally, the financial burden of stress is estimated to be $300 billion per year in the United States alone (American Psychological Association, APA Working Group on Stress and Health Disparities, 2017). As a result, there is pervasive and interdisciplinary agreement on the importance of understanding and alleviating stress to improve quality of life. However, the measurement of stress varies greatly within the large body of work linking stress and well-being. Researchers attempting to quantify stress should first understand the measurement strategies available to them and the strengths and limitations of each form of measurement. The goal of this paper is to define stress and offer an overview of measurement methods available to researchers interested in capturing stress.
Defining Stress
The definition of stress has evolved over several decades, and a universally adopted definition has yet to be reached. Seminal models of stress proposed by Selye in the 1950s define stress as the “non-specific response of the body to any demand for change” or the “rate of wear and tear on the body” (Selye, 1956). Proposed refinements to these definitions in the decades since have differentiated between stressors, defined as stimuli that challenge an organism’s biological and psychological equilibrium (i.e., homeostasis), and the stress response, defined as the process through which the organism attempts to restore homeostasis (Chrousos, 2009). Although the revised definitions differentiate between the cause and effect of stress, they have frequently received critique for being too vague, as nearly all activities that an organism undertakes constitute a challenge to homeostasis (Koolhaas et al., 2011). One model created to further clarify a working definition of stress, the psychophysiological stress concept, has been widely adopted in stress-related research since its dissemination in 2011 (Koolhaas et al., 2011). Developed by Koolhaas and colleagues, the psychophysiological model of stress defines stress as the perceived or anticipated inability to successfully cope with situations that are not predictable or controllable (Weckesser et al., 2019). This inability to cope with an experience leads to both subjective feelings of stress and objective biological changes in the body (Weckesser et al., 2019).
In defining stress, it is also important to recognize that stress can be conceptualized both as an acute reaction and a chronically accumulated state throughout the life course. Taken with the information above, this highlights three domains vital to the study of stress: (1) the presence of environmental stressors, (2) psychological and biological reactions to stressors, and (3) the length of time over which the stressor or stress response occurs (Monroe, 2008). Many subjective and objective measures have been developed and validated to quantify these domains. The following sections will cover not only subjective measures that capture perception of environmental stressors and psychological response but also objective measures that capture biological change.
Measures of Self-Report
Self-report measures of stress consist of series of questions or prompts that inquire about respondents’ lived experience with various components of stress. Several measures have been developed to quantify both reactions to acute stressors and the accumulation of chronic stress (Table 1).
Common measures to assess chronic stress include both the Life Events and Difficulties Schedule (LEDS) (Brown & Harris, 1978) and the Trier Inventory for Chronic Stress (TICS) (Petrowski et al., 2018; Schulz et al., 2004). The LEDS captures exposure to severe acute events (i.e., those lasting less than 1 month) and severe chronic difficulties (i.e., those lasting longer than 1 month) over the previous year through a semi-structured interview that prompts the individual to recall 95 possible life events. The individual provides additional context around each experience; a trained expert then codes the context. LEDS stressors are grouped into 10 domains: education, work, reproduction, housing, money/possessions, crime/legal, health/treatment/accidents, marital/partner relationship, other relationships, and miscellaneous. The TICS attempts to capture chronic stress through a more-structured questionnaire covering nine factors of chronic stress: "work overload, social overload, pressure to perform, work discontent, excessive demands at work, lack of social recognition, social tensions, social isolation, and chronic worrying. Participants in these surveys rate 57 items covering how often situations within the nine domains occur (i.e., never, rarely, sometimes, often, or very often) over a recall period of 3 months.
Several measures have been designed to capture stress over a shorter period of time, including the Cohen Perceived Stress Scale (PSS) and the Stress Overload Scale (SOS), among others (Table 1). The most commonly used measure for assessing global stress perceptions is the 10-item PSS (Cohen et al., 1983). This survey captures the degree to which a person views their life as uncontrollable, unpredictable, and overloaded in the past month. Scores are calculated using a five-point scale (0 = never, 1 = almost never, 2 = once in a while, 3 = often, and 4 = very often) that is summed for a total score, where higher scores represent a greater level of perceived stress. The PSS has been translated into a variety of languages (Lu et al., 2017; Remor, 2006), which allows for its use in both English and non-English-speaking populations. As an alternative to the PSS, the SOS was designed to measure when stress overwhelms a person’s coping mechanisms (Amirkhan, 2012). Twenty-four statements touch on personal vulnerability and event load, and an additional six items are used to discourage inconsistent responses. A shorter version of the SOS (10 items) also exists (Amirkhan, 2018). Each of the statements is evaluated on a 5-point graded-response scale (1 = not at all, 5 = a lot) to investigate feelings and experiences from the prior week.
Though measures such as the PSS or the SOS capture stress over a shorter time than measures of more-chronic stress, they are still frequently criticized for having great potential for bias because individuals are asked to report retrospectively on cumulative stress experienced. In response to this limitation, the ecological momentary assessment (EMA) method was developed. EMA is the repeated measurement of an individual’s subjective experience of stress in the context of daily life (Shiffman et al., 2008). This method can be used to capture momentary stress at multiple points throughout the day, which can then be aggregated to create a picture of stress levels over time. As technology has evolved, the smartphone has become a popular tool for conducting EMAs and contextualized survey items, including single-item measures (Yang et al., 2019). For example, a question prompted by a beep on a responder’s phone, such as “How stressed were you right before the beep went off?” can capture real-time stress with a variety of response options (not at all, a little, moderately, quite a bit, and extremely) (Jones et al., 2017).
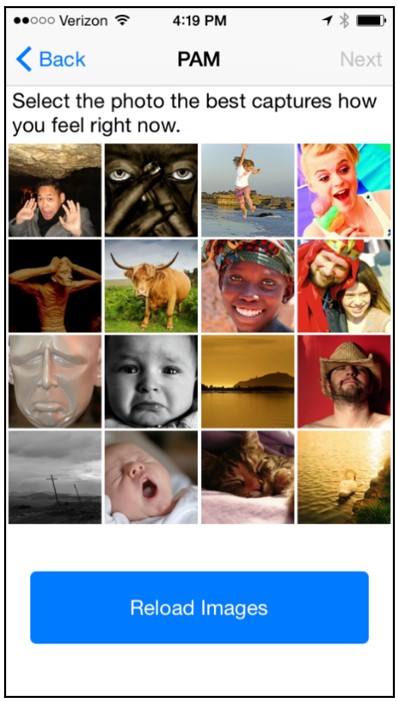
One measure used for EMAs is the Photographic Affect Meter (PAM). PAM is a validated, one-item, mobile application–based measure of affect that correlates with the widely used Positive and Negative Affect Schedule (PANAS) (Pollak et al., 2011). As shown in Figure 1, subjects select an image from a grid of 16 pictures that best represents their current emotional state.
.jpeg)
PAM is used to construct a set of numbers for the purpose of quantitative analyses. The first is a categorical 1–16 score that maps on to the PANAS scale (Watson et al., 1988). Consistent with the conceptualization of the PANAS, this affect scale ranges from low valence (the level of pleasure that an event generates) and arousal (the level of autonomic activation that an event creates) to high pleasure and arousal. Therefore, PAM also produces two separate affect scores for valence and arousal, which are calculated according to the chosen image’s position in the 16-image grid. Valence is computed using a 1 to 4 score (negative, slightly negative, slightly positive, positive) based on the column position of the image. Arousal is computed in a similar fashion using the row position of the image, with 1 representing calm or low arousal and 4 representing excitement or high arousal.
Self-report measures are useful tools in establishing subjective evaluations of stress levels. They are often cost-effective and correlated with clinical endpoints of interest, but they can be lengthy to administer and are subject to several types of bias (Demetriou et al., 2015; Nielsen et al., 2008; Razavi, 2001). Self-report measures are best used in combination with objective biological or digital markers of stress to understand the comprehensive impact on outcomes of interest (Weckesser et al., 2019).
Biomarkers
Stressors cause a variety of biological responses. These physiological reactions can be measured using biomarkers that represent the stress response from the hypothalamic-pituitary-adrenal (HPA) axis, the autonomic nervous system (ANS), and the immune system (Table 2) (Piazza et al., 2010).
The HPA axis is particularly responsive to psychosocial stress. One output of this system is cortisol, a hormone secreted from the adrenal gland that plays a vital role in cognition, metabolism, and immune function as well as the stress response. Levels of cortisol in the body fluctuate daily in response to routine events, unexpected stressors, and circadian patterns that render salivary cortisol highest in the morning and lowest at night (Hellhammer et al., 2009; Kirschbaum & Hellhammer, 1994). In addition to daily variation, cortisol may be chronically high or low. Both the acute fluctuation and the chronic compounding of cortisol are of interest to researchers. Acute cortisol change can be reliably measured in saliva and blood, cortisol in urine can be used to establish daily cortisol secretion (Remer et al., 2008), and cortisol in hair can be used to gather long-term cortisol levels over weeks or months (Wright et al., 2015). Salivary and hair cortisol are commonly used in studies investigating stress because collection is relatively quick and easy. Assessment of cortisol in saliva captures acute cortisol production over the past 15–20 minutes and is often used to measure daily stress.
Collecting saliva samples is comparatively easy and painless (a cotton swab is placed in the mouth of a participant and then sealed in a container), but a single saliva cortisol sample tells little about levels of stress over an extended period of time, and collection time is incredibly important, as cortisol levels vary across the day. Therefore, multiple samples of salivary cortisol throughout the day are needed to accurately capture daily stress. Cortisol levels measured in hair are used as a longer-term biomarker of HPA axis activity because cortisol is incorporated into the hair as it grows (Pragst & Balikova, 2006). Thus, hair cortisol captures a much longer period: a 1-cm hair segment reflects total cortisol secretion in the past month. These cumulative levels of hair cortisol do not provide information about HPA axis activity specific to any particular time within the measurement period.
The ANS modulates organ system activity through autonomic reflexes that respond to internal and external stimuli. Catecholamines, including norepinephrine and epinephrine, are hormones made by the adrenal glands that serve as strong biomarkers of ANS activity, specifically sympathetic-adrenal medullary (SAM) activity (Godoy et al., 2018). SAM activity occurs as a rapid response to a stressor to produce alertness and aid in responsive decision making. By contrast, HPA axis function is more representative of exposure to repeated stressors. Catecholamines can be captured acutely through blood concentration and as a short-term biomarker of daily stress through a 24-hour urine collection protocol (Baum & Grunberg, 1995; Remer et al., 2008). Alpha-amylase, an enzyme that breaks down starch, is another biomarker of ANS activity and can be detected in saliva samples (Ali & Nater, 2020). Like cortisol, epinephrine, and norepinephrine found in the urine, alpha-amylase fluctuates over the day, so multiple measures are needed to properly understand changes in alpha-amylase in response to stressors (Ali & Nater, 2020).
Another way to capture stress response is to measure immune activation (Segerstrom & Miller, 2004). Cytokines are a group of proteins that serve as signaling molecules that help mediate and regulate immune function and can be measured from blood samples (Segerstrom & Miller, 2004). Interleukin (IL)-6 is one type of cytokine that plays a vital role in the development of fever and regulates the acute inflammatory response in the liver (Cronstein, 2007). Although IL-6 is correlated with the development of cardiovascular disease and other chronic inflammatory disorders, it is very sensitive and easily elevated by exercise. When collecting samples, participants should refrain from exercise for approximately 12 hours to get an accurate reading.
C-reactive protein (CRP) is another substance integral to immune system response that is used to investigate stress (Johnson et al., 2013). CRP is made in the liver and released in reaction to inflammation, and it has been linked to stress response in humans. One advantage to using CRP as a measure of stress is that it lacks diurnal variation. However, CRP values can never be diagnostic on their own, and information about other pathological markers is vital to interpreting CRP levels.
Other immune measures of stress include the measurement of antibodies for common herpes viruses, including Epstein Barr virus antibodies, herpes simplex virus type 1 (HSV-1) antibodies, and cytomegalovirus antibodies (Glaser et al., 1985, 1991; McDade et al., 2000). These viruses are persistent infections that require adequate cell-mediated immunity to maintain in their latent states (Dowd et al., 2011; Herbert & Cohen, 1993). Longer-term stress can decrease the immune system’s ability to keep these viruses from reactivating (Dowd et al., 2011; Herbert & Cohen, 1993). As they reactivate, increased antibodies produced in response to circulating viral particles can be used as a measure of stress (Dowd et al., 2011; Herbert & Cohen, 1993).
The biomarkers listed here provide quantifiable measures of the various physiological pathways that lead to a biological stress response. The use of these biomarkers in stress research allows for a more-objective measure of stress and a deeper understanding of the alterations in biological systems caused by chronic and acute stress. However, researchers often assume the validity of biomarkers despite the need for continued evaluation (Strimbu & Tavel, 2010). Many stress biomarkers indicate levels of inflammation, but many factors influence inflammation, and they should be considered in the analysis (O’Connor et al., 2009).
The methods for obtaining biological samples for analysis may be a limitation for many researchers. Both the investigator collecting the samples and the participant need appropriate training because of the need for valid and consistent collection procedures (Djuric et al., 2008). Correct processing after sample collection, shipping requirements, and the proper storage of the biological samples are also critical for reliable results but can prove difficult in resource-limited areas.
Digital Measurement of Biomarkers
The use of sensors, software tools, and signal processing methods to explore complex biological signals related to stress has increased with recent advances in computational methods and concurrent, widespread adoption of consumer electronics (Schmidt et al., 2018).
Although a broad range of systems influence cardiac performance and functions, the ANS is the most prominent (Thayer et al., 2012). Like some of the aforementioned biomarkers, pulse and heart rate variability (HRV) can be used as proxies for fluctuations in the ANS in response to external and internal stressors. Pulse represents the arterial palpitation of the heartbeat and is reported in beats per minute. When individuals are exposed to stressors, their breathing and pulse can temporarily change. The alteration in heartbeat is measured through touch at any place where an artery can be compressed; two of the common areas for measuring pulse are the wrist and neck. HRV, or the fluctuating time between heart beats, can also be used as a proxy for ANS response to regulatory impulses and stress (Kim et al., 2018). Typically, when the ANS is stimulated, variation between heart beats is low, and during relaxed states, variability is high. Advantageously, fluctuations in HRV can be measured while other physiological markers of stress remain constant (Furberg et al., 2017).
HRV, as well as pulse, can be captured through different techniques with varying validity and convenience. Electrical impulses cause cardiac muscle to squeeze and pump blood from the heart, which can be captured through electrical leads attached to an electrocardiogram (ECG). The ECG method is the gold standard for measuring electrical activity of the heart. However, it is difficult to reliably collect ECG data in a cost-efficient, ecologically valid manner. In response to these challenges, wearable device manufacturers have turned to photoplethysmography (PPG) sensors. PPG is an optical measurement of blood volume variations as capillaries expand and contract with each heartbeat (Castaneda et al., 2018). Data collected using wearable PPG sensors has shown varied validity when compared with the gold-standard ECG (Bent et al., 2020). This is mostly because of differences in what PPG and ECG measure. PPG measures variability in peripheral pulse, whereas ECG directly measures the electrical cycles of heart function. Several factors, including blood pressure and age-related changes to the vascular system, influence peripheral pulse (Drinnan et al., 2001). Differing device quality and sensor placement can also explain differences between ECG and PPG. Placement is most commonly on the wrist, but can also be on the forehead, earlobes, upper arm, torso, fingertips, and ankles. Each of these locations experiences unique amounts of movement, which can limit the sensor’s ability to capture an accurate PPG reading. To counter the effect of movement on PPG sensors, wearable manufacturers are incorporating three-axis accelerometer data into their heart rate algorithms (Castaneda et al., 2018). As ECG and PPG wearable technology improves, large-scale health studies are producing robust, evidence-based results using user-owned devices (Perez et al., 2019).
Electrodermal activity (EDA) is another physiological measure of stress response that can be captured through sensor-based measurement (Garbarino et al., 2014; Liu & Du, 2018). EDA is the variation in electrical characteristics of the skin. These fluctuations in conductivity are caused by the changes in the ANS and are considered the most-useful index of ANS arousal (Furberg et al., 2017). EDA is measured through continuous monitoring of the involuntary changes in skin conductivity. EDA is particularly useful when assessing changing impacts of stress because of the continuous alterations in skin conductance (Reinhardt et al., 2012) and because it is the only ANS variable associated with psychosocial stress that is not correlated with other parasympathetic markers (Furberg et al., 2017). Researchers can capture EDA through wearable devices such as the Empatica (Garbarino et al., 2014).
Like biomarkers, sensor-based measures provide an objective method for quantifying the physiological response to psychosocial stress. Gathering complex, multisensory data on pulse, HRV, and EDA is easy and minimally invasive because of advances in technology. The development of small, reliable, and cost-effective biometric devices has created an increase in access and interest among consumers. However, these digital measures can only capture the stress response contemporaneously. In addition, the accuracy of some commercially available biometric devices is questionable, and assessment of the data quality is needed when using this technology.
Relationships Between Subjective and Objective Measurement of Stress
Subjective and objective measures of stress are related, but not identical, constructs. The psychological experience of stress may not always translate to measurable biological change and vice versa (Koolhaas et al., 2011). Limited research exploring associations between subjective and objective measures exists, and that which does suggests notable, but weak, associations between the two types of measures. For example, a recent study by Weckesser and colleagues found that only 16% of the variance in hair cortisol was explained by the subjective Weekly Hassle Scale, and that hair cortisol was not significantly related to the PSS or the TICS (Weckesser et al., 2019). In contrast, other studies have found statistically significant relationships between cortisol and the PSS (Walvekar et al., 2015), and other self-report measures such as the SOS (Amirkhan, 2012; Amirkhan et al., 2015) or aggregated subjective stress measures built from a combination of other measures (O’Brien et al., 2013). The relationship between perceived and objective measures of stress may be further explained by other factors, such as resilience. For example, a recent study by Lehrer and colleagues found that psychological resilience moderates the association between perceived stress (measured by the PSS) and hair cortisol; higher resilience reduces the association between perceived stress and hair cortisol (Lehrer et al., 2020). Further exploration of the relationships between self-report and objective measures of stress is needed to provide greater understanding of the impacts of stress on health.
Future Research Needs
Stress is a multidimensional construct that comprises exposure to events, perceptions of stress, and physiological responses to stress. A nuanced understanding of the links between stress and health requires assessment of each of these components in both acute and chronic scenarios. Employing self-reports allows for subjective evaluations of stress that illuminate the duration and severity of the psychological response to stressors. This information is vital to understanding the physiological stress response measured by biomarkers. Biomarkers, in turn, capture a more-objective measure of stress and create a deeper understanding of the biological response to chronic and acute stress. Finally, the use of digital biomarkers allows for further exploration of the physiological fluctuations caused by stress by measuring the changes occurring at the same time as the stressor. Future research should therefore favor a multidimensional approach that creates a triangulated picture of stress, drawing from perceived measures of stress as well as chemical and digital biomarkers. This will enable a more-comprehensive and holistic understanding of environmental stress triggers and corresponding psychological and biological responses.