Introduction
The World Health Organization and World Bank (2011) estimate that there are more than 1 billion people with disabilities in the world. To address this population’s diverse needs, the United Nations drafted their Convention on the Rights of Persons with Disabilities (CRPD) in 2006. Article 24 (Education) of the CRPD requires ratifying countries to develop an inclusive education system to address the educational needs of students with disabilities alongside their peers without disabilities. According to the United States Agency for International Development (USAID) (2018), inclusive education means:
Having one system of education for all students, at all levels (early childhood, primary, secondary, and post-secondary), with the provision of supports to meet the individual needs of students. Inclusive education focuses on the full and effective participation, accessibility, attendance, and achievement of all students, especially those who, for different reasons, are excluded or at risk of being marginalized. (p. 45)
As of December 2019, 181 countries have ratified the CRPD, which means those governments have committed to developing a system of inclusive education. This process can be complex because of the many financial and logistics barriers that countries, especially low- and middle-income countries (LMICs), face (United Nations, 2019). This commitment to inclusion has been reinforced by the United Nations Sustainable Development Goals (SDGs), where Goal 4 emphasizes the need to provide inclusive education to students with disabilities (United Nations, 2015). Developing inclusive education systems requires coordination across all levels of a system and requires coordination of government agencies that span education, health, social welfare, and early childhood. This development can only be accomplished if education systems tackle barriers such as policies that limit inclusion, discriminatory views toward disabilities, under-prepared teachers and inflexible curricula, lack of accessible learning materials, lack of appropriate identification and diagnosis systems and services, and inaccessible facilities (Hayes, Turnbull, et al., 2018).
This guide attempts to address one of these challenges: the lack of appropriate, useful disability screening and identification systems and services. As countries look to educate all students in inclusive settings, it is important to develop a system for screening, identification, and qualification for special education services that is based in the school and can be provided within an inclusive school classroom. Within such a school-based system, teachers should be trained and able to regularly screen students for disabilities. Additionally, qualified staff should be available to perform more-in-depth disability evaluations within the school environment. Although the availability of trained and qualified staff is not a reality in many LMICs, it is important that governments work to progressively to build capacity in this area.
Currently, most LMICs lack policies, protocols, tools, and expertise related to screening, evaluation, and qualification for additional services (Hayes, Dombrowski, et al., 2018). To address the need for disability identification services, many countries have established specific assessment centers as a way to provide at least some form of evaluation services. These centers typically exist in larger towns or cities, are intended to serve families across a broad geographic area who travel to the center for testing, and employ staff trained in an array of disability identification tests and processes.[1]
Although these centers appeal to many governments because of perceived cost-efficiencies, this centralization of identification services into a small number of discrete centers comes with challenges. For one, conducting identification practices in stand-alone centers means that a student’s identification is conducted over a shorter period of time—typically over one or two days—than is possible if working with a student in that student’s school. The shorter identification period does not give assessment center staff sufficient time to observe and determine a student’s abilities and support needs over time. In addition, identifying students in a center does not allow staff to observe a student across settings in the school or to meaningfully engage families as partners in the evaluation process. As a result, these identification practices often do not result in meaningful recommendations for instructional techniques that help both the teacher and the student. Further, the diagnoses given in these centers are often used as a justification to exclude students from, rather than include them in, mainstream schools. Because of these challenges and limitations, stand-alone assessment centers fail to promote the development of inclusive education practices around the world.
This guide provides guidance on moving away from the use of specific assessment centers to identify and diagnose disabilities. Doing so will help make education services more responsive to the needs of students with disabilities and more in line with CRPD guidance. Specifically, this guide
-
provides a brief background on the purpose and intended outcomes of identification,
-
describes the challenges of stand-alone assessment centers and the benefits of school-based identification practices,
-
provides practical steps for governments, donors, and practitioners on how they can build off of existing assessment strengths within a country, and
-
conceptualizes identification of students with disabilities as an educational service rather than a place.
Worldwide Situation of Identification of Students with Disabilities
Protocols and systems for identifying students with disabilities and determining whether they qualify for special education services vary dramatically worldwide. Some countries, such as the United States and Finland, rely heavily on the identification of a specific disability or set of disabilities in determining the education support a student will receive, and this reliance on identification is embedded in their national inclusive education laws (Björn et al., 2016). Unfortunately, many countries have also historically required students to have an official diagnosis to attend segregated, disability-specific schools, such as schools for students who are deaf or schools for students who are blind. For example, Belgium requires that children be assigned diagnostic criteria and medical labels before being able to attend a segregated school (Mortier & Vandelanotte, 2017). In some countries, children with suspected disabilities must also receive a diagnosis before attending inclusive schools. This trend of requiring a diagnosis as a precursor to school enrollment in both inclusive and segregated schools continues today in many countries, including China, Ghana, Greece, Kenya, Turkey, and Zimbabwe (Avoke & Hayford, 2017; Cavkaytar et al., 2017; Chitiyo et al., 2017; Deng & Wang, 2017; Kartasidou & Pavlidou, 2017).
In these countries, the diagnostic testing is often done in national or regional assessment centers. Core responsibilities of staff in these centers are to not only provide a medical diagnosis, which often results in recommendations for placement within segregated schools, but also decide whether students can be educated within inclusive classrooms. For example, Greece’s Centers for Differential Diagnosis, and Support for Special Education Needs are responsible for providing recommendations for educational placement (Kartasidou & Pavlidou, 2017). As a counterexample to this practice, Australia, Canada, and Finland are moving away entirely from diagnosis and instead focus on students’ needs rather than disability labels. In other words, these countries provide identification as a service rather than as a place and shift focus from diagnosis to inclusive in-class supports.
Although some countries are moving to a social model[2] when it comes to diagnosis, countries such as Malawi, Nigeria, Senegal, and Rwanda currently do not have existing formal systems of identification and rely on teacher discretion to determine a student’s eligibility for special services, or for placement in a segregated school (Drame et al., 2017; Itimu-Phiri et al., 2017; Karangwa, 2017; Obiakor & Eleweke, 2017). Too often, though, these teachers are not sufficiently trained in how to screen, evaluate, or determine necessary supports for students, especially those with disabilities such as learning disabilities that require more-sophisticated identification tools and protocols. In a similar vein, although Jordan has three official government-supported assessment centers, teachers are reported to develop their own tools and informally identify students as having disabilities (Research related to the results of the assessment centers in Jordan was not available) (RTI International, 2017). In at least one country, Uganda, assessment centers once existed but were discontinued (Okech, 2017). The article does not give reasons for the discontinuation or indicate what sort of identification services replaced the centers.
Countries also vary in where they place assessment and identification staff. Many LMICs rely on limited numbers of stand-alone assessment centers to conduct disability identification. Other countries, such as Australia, Canada, Denmark, England, Finland, New Zealand, Sweden, and the United States, assess students within the school setting to determine whether a student qualifies for additional services and supports (Arthur-Kelly & Foreman, 2017; Björn et al., 2016; Dyssegaard & Egelund, 2017; Gaffney et al., 2017; Killoran & Parekh, 2017; Patton & Wehmeyer, 2017; Rose & Qureshi, 2017; Wilder & Klang, 2017). In other countries, assessment center staff are not employed by or tied to individual schools but are available to support school-based assessment teams. In Brazil and Northern Ireland, identification is conducted within the classroom, but school teams have access to itinerant specialists to support screening and evaluations if needed (Kassar & Magario, 2017; MacKenzie, 2017).
Countries that provide identification as a service made available in schools tend to have the largest population of students educated within inclusive education systems. In Finland, less than 2 percent of students with disabilities are educated in segregated schools (Jarvinen, 2007), and less than 1.7 percent of students with disabilities in Sweden are segregated (Government of Sweden, 2012). Conversely, most of the countries with independent assessment centers continue to support segregated schools and have yet to implement inclusive education universally. For example, Turkey has 93 national assessment centers supported by 440 staff members, and most of students with disabilities receive an education in one of the country’s 480 segregated schools (Melekoglu et al., 2009). This number is exceedingly high compared to countries that only have a few assessment centers or do not have assessment centers at all.
Challenges of Assessment Centers
Although the appeal of instituting stand-alone assessment centers is notable—all funding and resources located and managed in a discrete number of centers—the reliance on assessment centers can limit access, constrain effectiveness, and even lead to misdiagnosis.
-
Lack of adequate tools and qualified staff. Although intended to offer comprehensive identification services, many assessment centers in LMICs do not have qualified staff, culturally adapted tools, protocols, or equipment needed to appropriately screen or evaluate students with disabilities. A lack of culturally adapted tools and qualified experts to administer screenings and evaluations can lead to misidentification and misdiagnosis (Oakland, 2009). The governments of Ghana, Senegal, and Jordan all cite experiencing these challenges within their respective assessment centers (Drame et al., 2017; RTI International, 2017).
-
Lack of school-based identification practices. Identification practices conducted in a center and away from a student’s school environment do not represent an accurate picture of students’ classroom-based academic needs and do not engage teachers throughout the process, making it hard for people to recognize a student’s needs and propose appropriate academic supports. An assessment center–based approach largely focuses on a child’s deficits, as it does not harness the child’s classroom-based strengths that can be used to meet academic challenges.
-
Lack of family partnership. During the identification process conducted in many of the assessment centers, parents are often not engaged as active participants, and tend to only be recipients of information or findings (Karasu, 2014). Actively engaging families in the process results in more-accurate identifications (Farrall et al., 2015). Furthermore, as assessment centers tend to be regionally based, they can be geographically inaccessible to many children with disabilities and their families, which can place an undue financial burden on families and children with disabilities (Mukuria & Korir, 2006).
-
Identification practices result in labels rather than helpful teaching techniques. Too often, assessment center–based evaluations label a child with a disability without addressing how teaching techniques or curriculum can be adapted to serve the student’s unique needs. Likewise, assessment center–based evaluations often look primarily at student deficits rather than strengths. A deficit-based approach to identification focuses on what students with disabilities cannot do, rather than what they can, and lowers standards for student learning, which can result in the implementation of less-effective learning strategies. Ideally, the identification process informs teachers, the school team, and families (Farrall et al., 2015). The idea is that this information will then be incorporated into the student’s Individual Education Plan (IEP) along with possible additional accommodations to support and improve learning.[3] For more on the benefits of strength-based approaches to special education, see Elder, Rood, and Damiani (2018).
-
Identification practices justify exclusion rather than promote inclusion for many students. Assessment center–based evaluations are often used to justify exclusion of students with more-complex disabilities and placement in a segregated school rather than in inclusive local school settings (Hehir et al., 2016). This segregated approach to identification does not encourage assessment centers to help develop inclusive tools for teachers in primary and secondary schools, nor to develop inclusive supports, services, and accommodations in the school the student would attend in the absence of a disability. School-based identification practices can also be used to justify exclusion rather than promote inclusion if used improperly. See the textbox on Education Assessment Resource Centers, which summarizes many of the obstacles currently facing LMICs related to center-based assessments, using Kenya as a case study.
The Importance and Benefits of School-Based Identification Practices
Having health care centers or community-based support for screening and diagnosis is important for early identification and early intervention and for supporting adults outside of the classroom environment. However, it is critical that assessments linked to school services, school placement, and eligibility for special education services take place in a school and/or classroom setting. As noted above, school-based identification allows teachers to focus on students’ academic strengths and needs while observing students in a variety of school settings over time. Outlined below are some other benefits of providing identification as a service rather than a place.
-
School-based evaluations are more likely to identify strategies and supports for more students. Conducting evaluations in the school makes it possible to assess all children in the school and school catchment area. Conducting school-based identification practices also allows for the identification of academic strengths and challenges. Such approaches can provide useful instructional techniques and recommendations for student support that move away from merely placing labels on students and toward addressing their in-class academic support needs. Classroom-based identification practices can also reduce the stigma of labeling students, and when done correctly, can help eliminate the challenges of misdiagnosis. School-wide evaluations can help to identify supports for students with high-incidence disabilities (e.g., auditory processing disorders, dyscalculia, dysgraphia, language processing disorders) that may otherwise go unidentified and unsupported, especially in LMICs (Abosi, 2007). Sæbønes et al. (2015) also suggest that classroom-based identification should not only be literacy- and numeracy-based but also include more aspects of a student’s school experience (e.g., social aspects).
-
Firsthand gathering of data. Directly observing a student in the school setting allows the evaluator to see the multiple educational settings (e.g., classrooms, playgrounds) that a student is exposed to on a daily basis. Direct observation allows the evaluator to propose strategies and interventions that can be directly applied to each setting. For example, local curriculum and classroom-based identification practices are at the core of ecological assessments. For more on firsthand data gathering, see the Focus on Practice textbox, which discusses ecological assessments.
-
Evaluations are contextualized. School-based evaluations allow schools to implement needs-based supports, as opposed to a diagnosis-based system, which can result in the student being placed in a segregated school with less access to high-quality education (Stough, 2003). School-based evaluations also allow teachers to directly observe students in their natural learning environments, thereby providing teachers with usable in-class instructional strategies, elevating teacher expectations for student learning, and promoting higher student academic performance (Heckman & Masterov, 2005).
-
Parental involvement. As noted by Fish (2008), a lack of parental involvement can lead to provision of inappropriate supports for students with disabilities. Students with disabilities and their parents should be considered experts on their experience with disability. Engaging students with disabilities and their families in the school-based identification process can be helpful in identifying strategies and approaches that will work best for the child with a disability (Rutland & Hall, 2013). If parents are not traveling long distances to assessment centers and have the option for a more-localized school-based identification, then the decreased distance can lead to more parent involvement.
Strategies to Transition Toward School-Based Identification
For the reasons stated above, identifying students with disabilities in the students’ school environments is preferred compared with only identifying students with disabilities in stand-alone assessment centers. For countries that may currently have existing assessment centers, we recommend that they transition to a school-based identification system that is more aligned with an inclusive education system. This transition can be done in a way that is cost-effective, builds on existing resources and experience, and addresses the gaps often associated with assessing students with disabilities outside of the classroom environment. This section provides a three-pronged approach toward transitioning toward school-based identification:
-
Shifting from focusing on diagnosis toward prioritizing school-based supports for students
-
Transitioning stand-alone assessment centers to serve as resource and support centers for schools, providing itinerant services, training, coaching and mentorship, and technical resources, and other services
-
Promoting a phased approach to identification that includes school-based vision and hearing screenings, universal screenings to identify learning needs, and ecological assessments
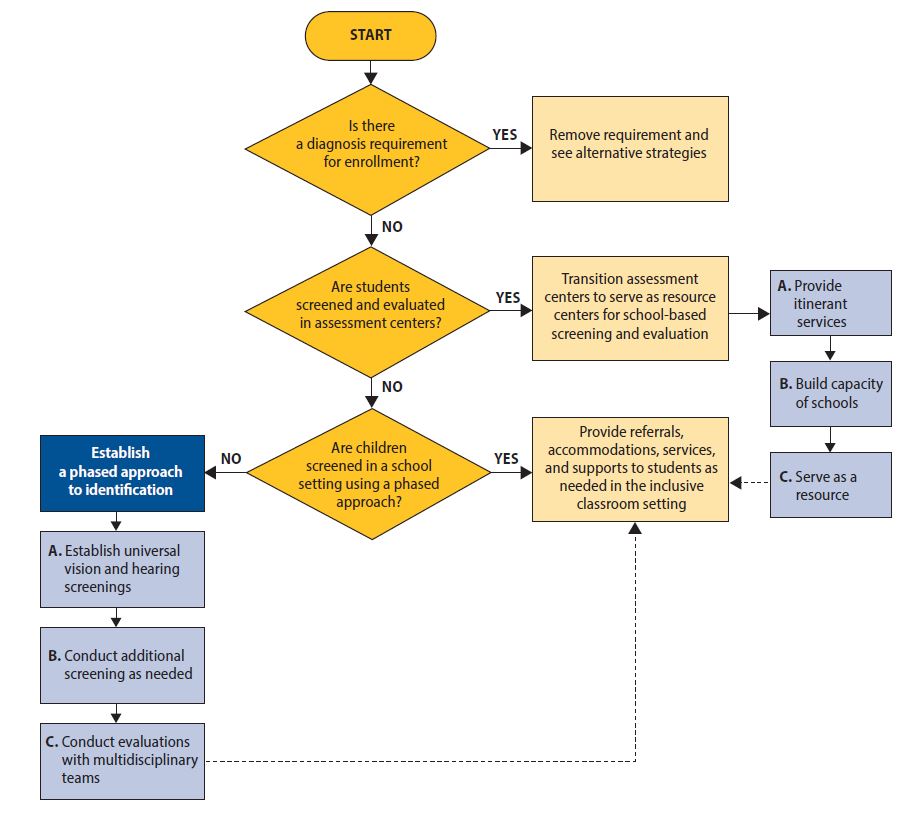
Educational systems can implement these actions over time while also supporting other initiatives for inclusive education. Figure 1 is a flowchart that clarifies the transition process. This flowchart takes readers through frequent questions related to screening and diagnosis and recommends next steps.

Transitioning from stand-alone assessment centers to school-based evaluations and support (i.e., making identification a service rather than a place) can be accomplished through progressive realization[4] and applying a phased approach. A phased approach allows schools to build upon current assessment strengths within a country, even a country with limited educational resources, while progressively addressing gaps in practices and becoming better aligned with international standards for best practices in inclusive assessment. The three suggested phases for assessment center staff are (1) providing itinerant support in inclusive classroom settings; (2) building the capacity of teachers and school staff through continuous training, coaching, and mentorship; and (3) serving as a temporary resource center for schools that supports referring families to community services.
Central to this transition is re-envisioning existing roles and responsibilities in ways that promote identification as a service rather than a place. This is extremely relevant in contexts that have limited resources for inclusive education; in these contexts, using the existing funding effectively is paramount. The information below outlines the phases and what may need to occur within each phase.
-
Provide itinerant services: Staff assigned to assessment centers should transition to supporting schools, where they should be tasked with conducting school-based identification services. Assessment center staff can initially serve as part of a multidisciplinary team, along with teachers and parents, to screen and support evaluations of students with disabilities in inclusive education classroom settings. Activities under this phase include the following:
\- Developing and implementing policies and protocols related to screening and evaluation. Although it is imperative to have policies and protocols to guide how and why students with disabilities are identified in an inclusive setting, establishing symbolic policies and laws without having ways to implement them is ineffective. After creation, policies and protocols must be regionally applied, implemented, and supported by governments. This requires that school system pilot tools and tailored them to cultural norms before being used at a national level. Additional training and guides on how to use the tools may also be needed.
Inclusion committees should be made up of stakeholders in inclusive education (e.g., students with and without disabilities, teachers, administrators, parents of students with and without disabilities, representatives of the Ministry of Education, and community members with and without disabilities). The committee should set goals and objectives and collectively work on them. Committees should regularly monitor progress to ensure results are directly benefiting students with disabilities and their families (Damiani et al., 2016; Elder & Kuja, 2018).
b. Reallocating budget for new assessment centers toward itinerant, training, and resource expenses. Most LMICs have limited funding for education and even fewer resources for inclusive education. Available funds must be spent wisely and allocated to efforts that promote inclusion. The CRPD Committee guidance on implementing inclusive education explicitly states that countries cannot maintain segregated parallel systems and remain in compliance with the CRPD (United Nations, 2016).
Shifting funding from maintaining and growing center-based assessment toward developing school-based identification service is part of the essential reallocation of resources that systems must undertake to promote full inclusion. For example, initial funding that might have been used to build additional stand-alone assessment centers can be reallocated to support travel for assessment staff to serve as itinerant assessment teams and train and support schools to conduct their own assessments.
c. Teaching parents, students, and communities about the value of inclusive education and school-based identification practices. Stakeholders in inclusive education need to be educated about the benefits of inclusive education and why and how identification for services should take place. Misunderstandings of what disability is and stigma surrounding disabilities within communities make the development of segregated schools seem justified. Therefore, making communities aware of topics related to disabilities, such as the legal imperatives of inclusive education (Elder & Kuja, 2018), is critical in the development of inclusive school-based identification practices.
As part of this process, assessment center staff can play a vital role in collaborating with families, teachers, and administrators in segregated schools, as well as teachers and administrators in local primary/secondary schools, to identify the placement of students transitioning from segregated schools into primary/secondary inclusive schools. Because parental rights will be different within each country, it is important that information and education for parents on the identification process policies and practices is country-specific.
- Developing and implementing policies and protocols related to screening and evaluation. Although it is imperative to have policies and protocols to guide how and why students with disabilities are identified in an inclusive setting, establishing symbolic policies and laws without having ways to implement them is ineffective. After creation, policies and protocols must be regionally applied, implemented, and supported by governments. This requires that school system pilot tools and tailored them to cultural norms before being used at a national level. Additional training and guides on how to use the tools may also be needed.
-
Build capacity of teachers and school staff through training, coaching, and mentorship: Assessment center staff’s knowledge, skills, and expertise will be critical throughout the transition to support school-based identification practices. They can share their expertise with teachers and school teams as those teachers and teams begin to implement identification practices directly within classrooms. Assessment center coaches and mentors can also share expertise on an ongoing basis as they collaborate with school teams to begin the new identification process. In addition to these supports, assessment center staff can support systematic change through the following activities:
\- Training teachers on student identification and qualifications for services. Because all teachers have students with disabilities in their classroom, it is important that all teachers are prepared as student teachers to conduct screenings and serve as part of a multidisciplinary team for evaluations. Ideally, special education teachers will also be available to lead this process and would need to receive additional training on best practices related to identification.
Similarly, after teachers are employed they must receive regular and ongoing training related to inclusive education and evaluation practices (Forlin, 2001). This training can come from assessment center staff, nongovernmental organizations (NGOs), and others, and should be a part of core in-service trainings.
b. Developing and revising identification tools as needed. Screening and evaluation tools need to be tailored to reflect the cultural norms of the environment in which they are used. This may require developing of new tools, refining existing tools, or both. Staff coming from assessment centers can use their expertise to help develop, pilot, refine, and revise tools as needed before implementing them at a national level within classrooms. All new or adapted tools should be validated with children with disabilities in the new context.
Such a refinement process would require that assessment center staff have access to evaluations that are easily adaptable to any environment and can be implemented with existing school resources (e.g., paper and pencil). For more information on these types of adaptable inclusive identification practices, see USAID’s Toolkit on Literacy (Hayes, Turnbull, et al., 2018).
- Training teachers on student identification and qualifications for services. Because all teachers have students with disabilities in their classroom, it is important that all teachers are prepared as student teachers to conduct screenings and serve as part of a multidisciplinary team for evaluations. Ideally, special education teachers will also be available to lead this process and would need to receive additional training on best practices related to identification.
-
Serve as supports and resources for referring families to community services: Even as education systems transition to providing identification practices as a service rather than a place, assessment center staff will have a role within the newly revised system. This repurposed role will allow individuals with experience and skills in this area to serve as a resource for classroom-based teams as needed. This role can include providing ongoing professional development to schools and families, answering questions and providing support related to challenges that school teams may have, continuing to strengthen tools as needed, and serving as a resource to refer families to existing community services that may be helpful for students who would benefit from additional services or access to assistive devices. Additional support from the resource center can include the following:
\
1. **Developing and maintaining community referral options.** Throughout the identification process, additional referrals may be needed. Such referrals can include more-detailed vision and hearing testing conducted by medical experts, access to assistive devices, and additional community supports and therapies that may not yet be offered through the school systems. Assessment center staff are in a unique position to collect data, update and maintain information on additional community resources and referral options, and share this information with schools as needed. It is important to note that all school placement options should be the decision of the parents and students with disabilities and not be made by the assessment center or the government.\
\
Likewise, for an educational system to be truly inclusive, all students with disabilities should be allowed to attend their local schools, and the referral process should not include recommendations to attend segregated schools. The only exception is education for students who are deaf. The World Federation of the Deaf (2018) defines inclusive education as the ability to interact directly with their peers and their teachers, which means being in a communication-rich environment that uses local sign language.\
\
b. **Reallocating school resources.** Conceptualizing inclusive education as a service rather than a place can help shape thinking about how formerly segregated school resources are reallocated (Theoharis & Causton, 2014). Inclusive education does not necessarily mean that more money needs to be spent supporting students with disabilities (Van Dyke et al., 1995); rather, it means thinking creatively about support and resource allocation. For example, if dormitory aides and instructional aides were formerly paid to help support students with disabilities in segregated schools, they can work at the inclusive school in their local area, for example helping families transport their children to school and work in inclusive classrooms.\
\
Governments can also provide incentives to parents to take their children with disabilities to the schools they would attend in the absence of a disability. Such incentives could include subsidizing transport for aides and students to and from school, providing free or reduced-price school uniforms, providing partial or full vouchers for school fees, and providing food subsidies.\
\
c. **Supporting uploading data from identification into the national Education Management Information System (EMIS).** Although a specific diagnosis is not needed to provide instruction for students, having data on the number of students who qualify for special education services can be useful for a variety of reasons. Having disability data can help inform national budgets, inform the need for assistive technologies, identify background information for students who are "at risk," and support the monitoring and evaluation of interventions (Croft, 2013).\
\
School systems can collect such data through household surveys and census information as well as through EMIS. It is therefore recommended that questions related to disability, accommodations, accessibility, and inclusion be added to a country's EMIS. For more information on how to include students with disabilities in EMIS, please visit the United Nations International Children's Emergency Fund's (UNICEF) (2016) [Guide for Including Disability in Education Management Information Systems](http://training.unicef.org/disability/emergencies/downloads/UNICEF_guide-for-including-disability-in-education-management-information-systems.pdf).
Identifying Students with Disabilities Within a School-Based System
As education systems transition to school-based identification and diagnosis of disabilities, schools can review and strengthen their identification and diagnosis processes and tools. The purpose of identifying students with disabilities in the school is to assess possible learning challenges, learning strengths, and types of services or supports that students may need to reach their full academic potential. Information and insights obtained through this process can help inform instructional techniques, accommodations, assistive technologies, and other methods to help students receive an inclusive education. The purpose of identification is not to label a child as having a disability without providing additional supports or to use information obtained through the identification process to justify exclusion. Rather, the purpose of identification and diagnosis should solely be to identify the most-effective learning supports for a student.
Ideally, identification should use a phased approach, be conducted within the classroom and school setting, include a multidisciplinary team of professionals, and engage families throughout the process (Hayes, Dombrowski, et al., 2018). This phased approach can be implemented over time at a pace that is manageable within the resources available to an education system. Systems that are struggling to find or reallocate resources can focus on implementing low-cost vision and hearing screening in schools, while systems that have more resources or are farther in their journey to inclusive education and have already addressed vision- and hearing-related disabilities can explore how to screen for other types of disabilities and strengthen referral and support systems for students who are struggling to learn (see, for example, Hayes & Bulat, 2017).
The recommended phased approach for screening and identification is as follows:
-
Phase 1. Establish school-wide vision and hearing screenings for all students: All students should receive routine vision and hearing screenings in a classroom setting. Screeners should refer students for additional screenings or supports if needed. Vision and hearing challenges must be ruled out before conducting additional screening and evaluation (Friend & Bursuck, 2018). After the screenings, students who are determined to need further testing should receive a full vision and hearing test from a qualified professional and then receive the necessary supports (e.g., hearing aids, glasses).
-
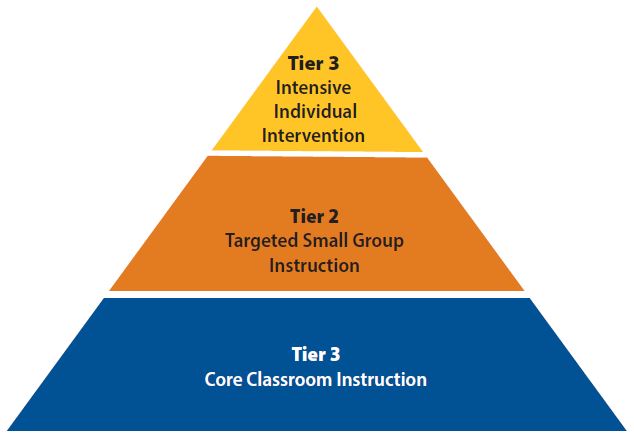
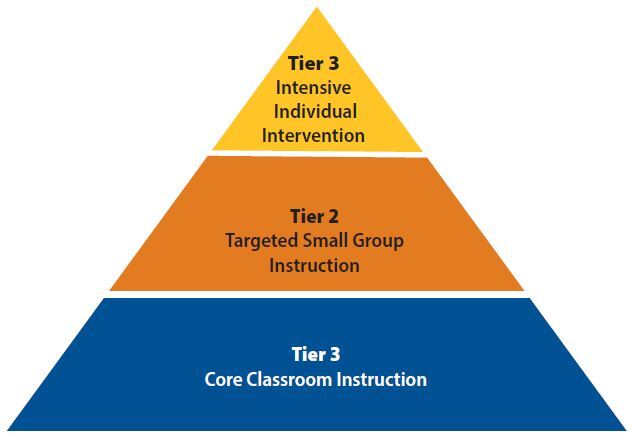
Phase 2. Establish screenings for other learning needs: Even after ruling out vision or hearing challenges, many students may continue to struggle to perform academically in the classroom and require screenings to assess whether they would benefit from additional teaching supports and special education services within the inclusive classroom setting. One of the most-effective screening approaches is Response to Intervention (see textbox), which uses systematic and evidence-based activities to determine additional learning needs. This method is often preferred over other methods, as it allows for all students to be screened and proactively provides targeted interventions for those who are struggling academically.
-
Phase 3. Establish evaluations with multidisciplinary teams: Students who continue to struggle academically and those who have a suspected or known disability need a more-comprehensive evaluation to identify underlying causes. This evaluation should be conducted by a multidisciplinary team and be used to determine a student’s academic, behavioral, and social strengths and challenges. Information from this evaluation can help determine whether a student would benefit and qualify for special education services as well as inform possible instructional approaches and accommodations that should be listed within a student’s IEP. One effective method for evaluations is using an ecological assessment. Ecological assessments compare students with possible disabilities to other same-aged peers within their classroom and consider some of the teaching or environmental varies that may be influencing students’ progress. See the Focus on Practice textbox for more information on ecological assessments.
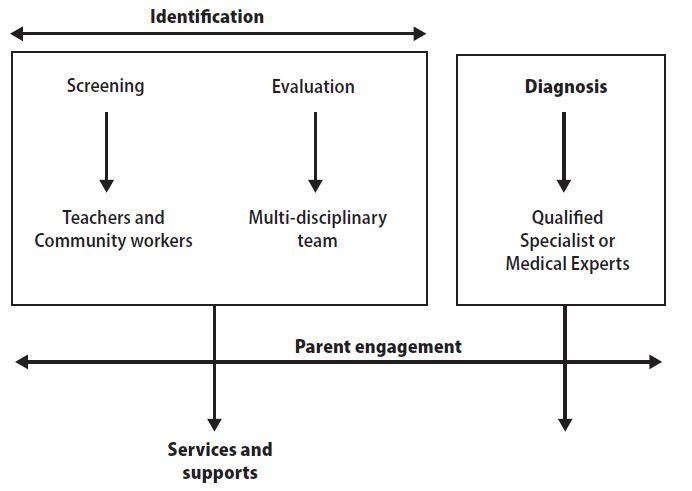
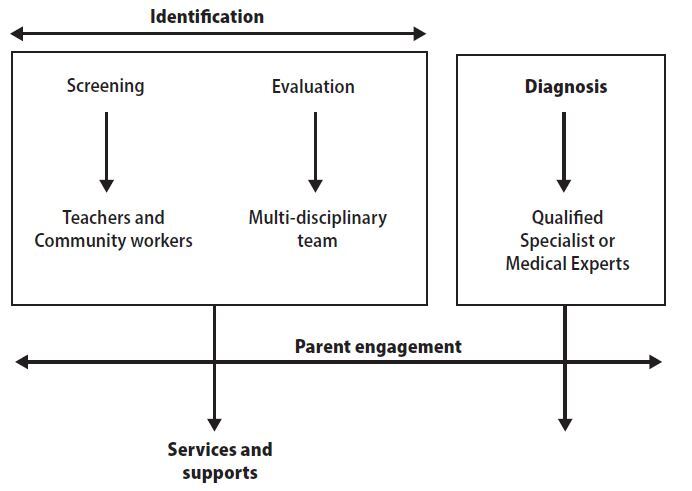
The phased approach outlined above is often poorly understood worldwide. Common errors include using screening techniques (with no formal evaluation process) to identify students as having a disability; using non-adapted or non-validated identification tools; not fully engaging families; and not conducing screenings or evaluations in the school or classroom setting (Hayes, Dombrowski, et al., 2018). Likewise, too often the focus of identification emphasizes providing a label or diagnosis rather than focusing on the individual student and the academic support that they may need. There is also often confusion on who is qualified to screen students versus provide a diagnosis. Although screening can be done by community workers and teachers, diagnosis should only be done by trained professionals or medical experts. Figure 3 provides more information on the different roles of this process.
Conclusion
Identification and eligibility for special education services are core elements of any inclusive education system. Ideally, school-based identification provides students, teachers, the school team, and parents with insights, knowledge, and tools on how to utilize students’ strengths while providing additional supports to address potential challenges. These supports then help facilitate academic instruction within an inclusive classroom setting. Unfortunately, many countries that are working toward implementing an inclusive system continue to support identification systems that are more aligned with segregation than inclusion. As part of a country’s transition toward inclusion, a country should reform its identification systems to support school-based identification practices. Especially where resources are limited, such as in LMICs, this proposed process can take place gradually while building upon and refocusing existing resources and slowly filling possible gaps in services. Identification systems that are solely diagnosis-based without observing students in the classroom setting do not engage families and often result in recommendations for student placement in segregated settings, which directly contradicts to the principles of the CRPD. Therefore, recognizing student identification as a service rather than a segregated place (e.g., assessment center) is paramount to achieving universal inclusive education that is aligned with the CRPD and the sustainable development goals.
Acknowledgments
The authors would like to thank their international educational partners who have who have generously opened up their schools and introduced us to their wonderful teachers and students without whom this work would be impossible.
In this report, we consider anyone who has paid interactions with students and families (e.g., assessment center employee) as “staff.” We consider certified teachers, specialists, and administrators as “professionals.”
The social model of disability recognizes that disability is part of the human condition and that persons with disabilities have the same human rights as persons without disabilities. The social model also locates disability in inaccessible societal spaces that create disability (i.e., curbs without curb cuts, television without captions). This is different from the medical model, which approaches disability as something that needs to be cured or fixed, or the charity model, which views disability as something that needs charity or pity.
An IEP is an educational plan that sets academic goals for students with disabilities and highlights what types of supports, accommodations, and additional services they may need to reach their full academic potential. Versions of IEPs are used in many countries throughout the world.
According to Article 4, Section 2 of the CRPD (United Nations, 2006), “Each State must take measures to realize economic, social and cultural rights progressively, using the greatest amount of available resources to do so. This obligation, commonly referred to as progressive realization, acknowledges that it often takes time to realize many of these rights fully, for example, when social-security or health-care systems must be created or improved.”